With confirmation that 2023 was the warmest year on record (between 1.43-1.48C above preindustrial levels depending on which dataset you use), it’s reassuring to read that the World Health Organisation is starting to take climate change seriously. In this post, I want to think about how WHO is communicating this challenge and what practical steps it is doing or needs to be doing.
A good place to start is with two recent documents from WHO’s Secretariat in preparation for its upcoming Executive Board meeting – Draft fourteenth general program of work (EB154/28 21st December 2023) and Climate change and health: Report by the Director General (EB154/25, 20th December 2023).
WHO’s primary strategic document is its General Program of Work, so it’s significant that of six objectives described within its draft 14th GPW, the first on the list is climate change. Objective 1: “Respond to climate change, the greatest health threat of the 21st century”. The word ‘climate’ appears 47 times in this draft (compared to 19 times in its previous GPW). Of course, just repeating a word more times doesn’t demonstrate increased commitment: Nevertheless, it is noteworthy. While it’s great to see the health impacts of climate change given such prominence, I think there are two big issues to consider even before we get to the practical steps of responding to it.
1: Language matters
I won’t quote paragraph 2 in full but here’s the headline: “The pace of climate change and environmental degradation has accelerated, emerging as the greatest threat to human health in the 21st century”. It doesn’t help to lump two phenomena together – climate change and environmental degradation – because it becomes unclear whether the acceleration refers to both separately or only when combined. Furthermore, if climate is by definition a statistical average of weather, does it make literal sense to state that “climate change” has a pace which has accelerated? What does that mean? Anyone familiar with the work of Ilan Kelman will know that I’m not just being pedantic here. Language matters, as Kelman argues in this very though-provoking presentation. I’ll return to Kelman’s work later.
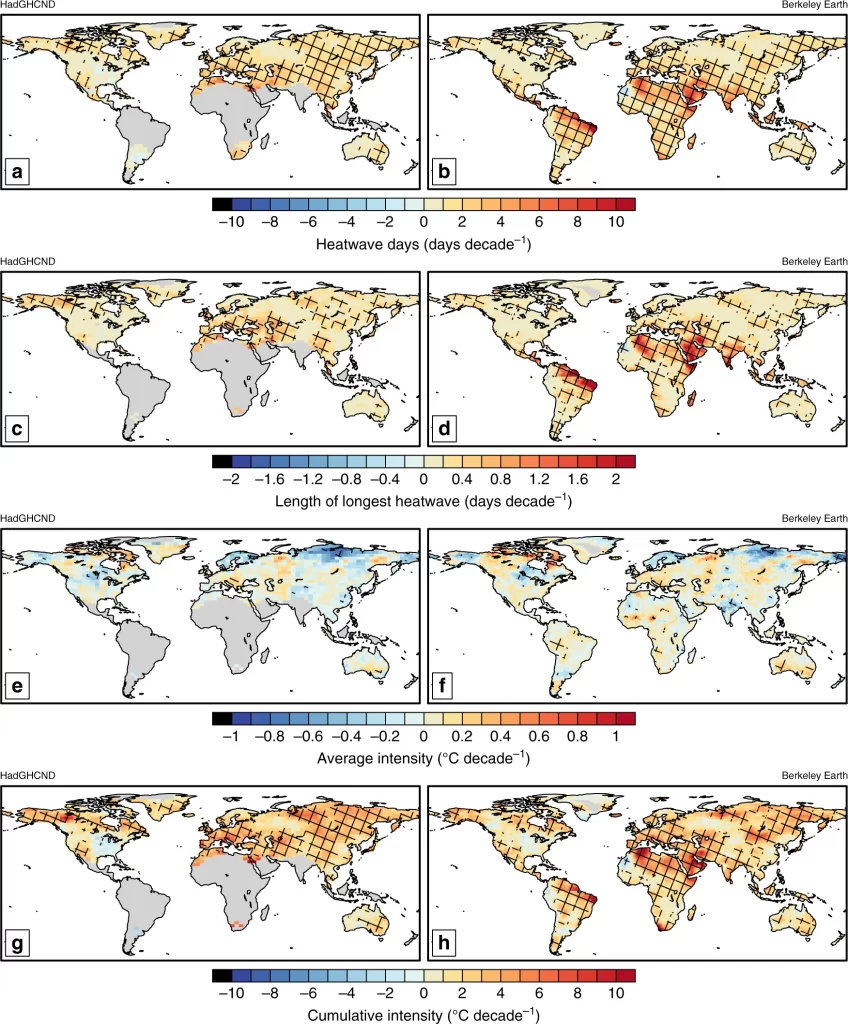
But to clarify what it means when we say that climate change is accelerating, we could start with global warming. We know unequivocally that the planet has warmed significantly in a very short period of time and that humans are responsible for 100% of that heating. Climate with respect to specific weather events – heatwaves for example – is changing. If heatwaves on average are hotter in the 2020s than they were in the 1980s, then there’s a change that we can quantify (a rate). If heatwaves on average are even hotter in the 2060s, and the change (rate) between the 1980s-2020s and the 2020s-2060s increases, then we can say that the rate of climate (with respect to heatwaves) change is accelerating – it’s speeding up (thanks to Ilan for clarifying this for me – calculus is not my strong suit. See here for more on calculating rate of change, if it’s not your strong suit either). Are heatwaves getting hotter? Yes. As temperatures increase, some (though not all) weather hazards (heatwaves, heavy precipitation, droughts in certain regions) are becoming not just more intense, but also longer in duration (AR6 WG1 SPM B.2.2) (see Figure below). Furthermore, as James Hansen has argued recently, global warming is also accelerating.
Unsurprisingly, it’s very difficult to quantify the excess mortality that is directly attributable to climate change. WHO’s 2014 quantitative risk assessment of “approximately 250 000 additional deaths due to climate change per year between 2030 and 2050” is (incredibly) still the benchmark. It’s likely a conservative estimate, not least because it focuses on selected health outcomes sensitive to climate change. Recent analysis focusing on just heat-related mortality by Bressler (2022) suggests that a baseline scenario where the planet heats to 4.1C by 2100 would result in 83 million cumulative excess deaths.
Both the WHO and Bressler give us a sense of the scale of the problem. For example, the WHO report notes: “Compared with a future without climate change, the following additional deaths are projected for the year 2030: 38 000 due to heat exposure in elderly people, 48 000 due to diarrhoea, 60 000 due to malaria, and 95 000 due to childhood undernutrition”. To make a couple of obvious points, while directly attributable excess deaths are high (and will increase as temperatures increase), these figures are still relatively small compared to other causes of death. For example, as Bressler points out “By the end of the century, the projected 4.6 million excess yearly deaths would put climate change 6th on the 2017 Global Burden of Disease risk factor risk list ahead of outdoor air pollution (3.4 million yearly excess deaths) and just below obesity (4.7 million yearly excess deaths). Furthermore, the excess deaths are relatively small compared to the total deaths – 1.5 million people died from diarrheal diseases in 2019, for example. One final point: through political decisions and action, the number of excess deaths directly attributable to extreme weather events exacerbated by climate change could be reduced significantly. Bressler notes that policies enacted now (with accompanying immediate action) that lead to 2.4C of heating by 2100 would reduce the 83 million excess deaths to 9 million, thereby saving 73 million lives.
Given the methodological challenges of quantifying and attributing mortality (and morbidity – ill-health is not just about death) caused directly by extreme weather events exacerbated by anthropogenic global warming (an increase in the number of deaths from heat stroke, for example), quantifying and attributing indirect mortality (heat reduces agricultural productivity and people starve to death following catastrophic crop failure) and, further, mediating or tertiary effects (farming communities begin to migrate and some perish in the process), is even harder. But it is likely these indirect and mediating effects are the ones people have in mind when they imagine the future impact of extreme weather events on health. Conceptually and empirically, though, we are – I think – just beginning to articulate the associations between extreme weather events and health at primary/secondary/tertiary levels.
2: Attribution – don’t shoot the messenger!
The second issue draws on another insight from Kelman. Climate change is a persistent, enduring, natural and neutral phenomenon which is being rapidly and significantly affected by human action, with devastating consequences. It’s that affect by us that is causing all the problems. And it’s our (current) failure to respond appropriately, our (current) failure to make the right social, economic and political choices – not climate change per se – that we should be focusing on. So when WHO declares “climate change is the greatest health threat of the 21st century” it is shooting the messenger. Worse, it’s doing the person who sent the messenger (we did) a favour because they/we remain in the shadows, absolved from their/our responsibility. From a communications perspective, it’s a much harder sell for WHO to persuade people that they can change climate change (how can we do that, it’s the climate!) than to call out the actual perpetrators of change (us) that we need to (and can) do things differently. You want a different climate, then create a less extractive economy; you want a different climate, then design and implement radical emissions reduction targets; you want a different climate, then seek peace instead of war. But don’t blame the climate!
There are a couple of things WHO could do here: 1. It could drop the shorthand term ‘climate change’ and use more cumbersome (but more precise) phrases such as ‘extreme weather events made more intense, frequent and longer-lasting by anthropogenic global warming’; 2. it could refrain from, or at least reflect further on, making statements that are hard/currently impossible to support with data. This is especially important in strategy documents such as the GPW because statements such as these set the tone for the discourse within the institution. And finally, 3., one practical thing that WHO should be doing is making the case for, and then supporting, primary data collection – particularly in those areas most at risk. Primary data on climate and health is fundamentally important, and yet many/most countries have partial/incomplete/out of date data with little resources or capacity to collect or update it on a regular basis.
These are just some initial points to consider when interrogating the claim from WHO that “The pace of climate change and environmental degradation has accelerated, emerging as the greatest threat to human health in the 21st century”. The GPW is an important document, and so it’s important to get the language right. The same is true for reports issued by WHO’s DG Dr Tedros – reports such as Climate change and health: Report by the Director General (EB154/25, 20th December 2023).
An existential threat?
The DG report refers twice to “the existential threat of climate change”. I’ve often used this kind of language – in previous posts, for example – but am much more cautious using it these days. Not because I think that the threat from extreme weather events caused by anthropogenic global warming/heating is diminishing, but because on balance I’m not sure it helps and can lead to ‘doomist’ thinking. First let me quote the DG report in full, so you can see the phrase in context:
“WHO is proposing to continue to lead the global health community, in partnership with other international health actors, to raise ambition in addressing the existential threat of climate change”.
A good review paper by Colin Butler and a very useful conceptual paper by Huggel et al help to understand the extent to which such threats are represented (or not) in the health literature, and also to provide a clearer and more nuanced definition of ‘existential’ risks. Here is Huggel et al’s definition:
Existential risks in the context of climate change are “those risks that threaten the existence of a subject, where this subject can be an individual person, a community, or nation state or humanity. The threat to their existence is defined by two levels of severity: conditions that threaten (1) survival and (2) basic human needs”.
In assuming the existential threat of climate change, WHO is potentially positioning itself at odds with the climate science community, which has not widely adopted the ‘existential’ narrative (although the IPCC’s ARG WG2 does explicitly refer to existential risk in relation to the risk of sea level rise to SIDS, loss and damage, and relocation), preferring instead the term ‘Reasons For Concern’ (RFC). The consequences of ‘large scale discontinuity’ (to use the slightly chilling euphemism used in the climate science literature) from RFCs is poorly understood, though. From the climate movement perspective, existential threat implies a need for global systemic change, notably economic change (with a specific critique of capitalism). How WHO interprets existential threat, therefore, seems important in terms of buy-in from both of these communities.
Huggel et al argue that the “extent a subject is affected by an existential risk depends on the hazard, and its exposure and vulnerability, and can vary among and between individuals, communities, countries, and regions”. In other words, it is not limited to the terminal asteroid impact type event that can wipe out all life on the planet. Understanding all-life-ending global catastrophe, and planning for such eventualities should not be off-limits. Kemp et al (2022) argue as much, even providing a useful, if bleak-sounding research agenda: “Extreme Earth System States, Mass Mortality, Societal Fragility, and Integrated Climate Catastrophe Assessments”.
Looking beyond the end of the world scenario, Huggel et al’s framework provides six dimensions of existential risk to guide the specificity of the threat: (1) the processes and mechanisms of threat, (2) systems affected by existential risk, (3) the magnitude of threat, (4) the probability of occurrence of the threat, (5) the time horizon, timing, and speed of the process, and (6) the scale. WHO could usefully apply these dimensions in its own work. Crucially, though, it needs to explain much more clearly what it means by the term ‘existential threat’ to its primary constituencies – especially its MS, the climate science and social science communities, and activists (of all ages).
What then is to be done?
Here’s a list of the “radical action” proposed by Tedros that WHO will deliver “to safeguard the health of the planet”:
- “further develop and scale up the application of existing climate change and health work across its core functions”;
- “provide the essential leadership, evidence, monitoring and technical support functions to guide the global health response”;
- “advance evidence-based messages, use communication science to present health as a positive and compelling argument for climate action, and accelerate the growing mobilization of engaged health professional and civil society organizations behind that agenda”;
- WHO to become carbon neutral by 2030;
- “Convene global experts”, compile “summaries of global and regional evidence”, “improve access to knowledge and data”
- “build on over a decade of experience in executing major projects on climate change and health, to provide assessment, planning and implementation support directly to those countries and populations most impacted by the climate crisis”.
- “facilitate access to finance from both climate and health funds, and work with partners to develop a co-financing facility specifically for climate and health”.
- “leverage and multiply its own efforts by working in effective partnerships, including leading the secretariat of the Alliance for Transformative Action on Climate and Health”.
I’ll leave it to you to decide whether you regard these actions as ‘radical’. It’s a fair list, but quite generic (as you might expect from an EB report) and vague on the details (let’s see more concrete and time-bound actions of the ‘by x date, WHO will have done y’ similar to point 4 on the list). I’m not going to pour cold water on all the efforts WHO is doing to raise the profile of health within the climate community: I’m grateful for those initiatives. In addition to these though, as noted above, I think WHO should be investing in conducting, or at least explicitly supporting, primary data collection. It also needs to explain its position on existential threats, especially considering the high-level focus it now has on climate change and health. But more than that, I’d like to know what its budget is for all of the above. There has never been a budget line in any previous Program Budgets for this work, and there’s no hint of how future work is going to be funded. So, the question we should be asking is how much money does WHO have “to safeguard the health of the planet”?
Andrew
Also read this excellent Commentary on EB154/25 on PHM’s Tracker website
https://docs.google.com/document/d/1ykIziZZFCDvoBbm8MfPPTRI6ikky-ZO68W0GVI3JVhQ/edit#heading=h.l4oz4d16iykl